ACORD™ 131
Commercial Umbrella
Get to know the ACORD™ 131 — the companion form to ACORD™ 130, used to detail Employers Liability coverage as part of your Workers Compensation submission.
PAGE 1

Form Key
1. Umbrella/Excess Section
ACORD 131, Umbrella / Excess Section, captures information about a liability coverage affording high limit excess and/or extended coverage. It is a separate policy over and above other basic liability policies the same insured may have. A completed Umbrella / Excess Application consists of both the Applicant Information Section, ACORD 125 and the Umbrella / Excess Section, ACORD 131. This is necessary because some information about the applicant is only shown on the Applicant Information Section.
2. Agency, Carrier, Policy Number, Effective Date and Named Insured(s)
Enter Agency Name, Carrier Name, Policy Number, Effective Date and Name of Insured(s).
3. Policy Information
Check the box for the applicable transaction type. Provide retroactive date if applicable. Provide limits of liability and retained limit.
4. Employee Benefits Liability
If Employee Benefits Liability coverage is in place, provide the Limit of Insurance, Aggregate Limit, Retained Limit, Retroactive Date and Name of the Benefit Program.
5. Primary Location & Subsidiaries
Provide the name and location of the primary and all subsidiary companies, describe their operations and provide their annual payroll, annual gross sales, and # of employees.
6. Underlying Insurance
List all Liability and Compensation policies in force to apply as underlying insurance. Provide carrier name and policy number, policy effective and expiration date, Limits, annual renewal premium and any rating mods.
PAGE 2
Form Key
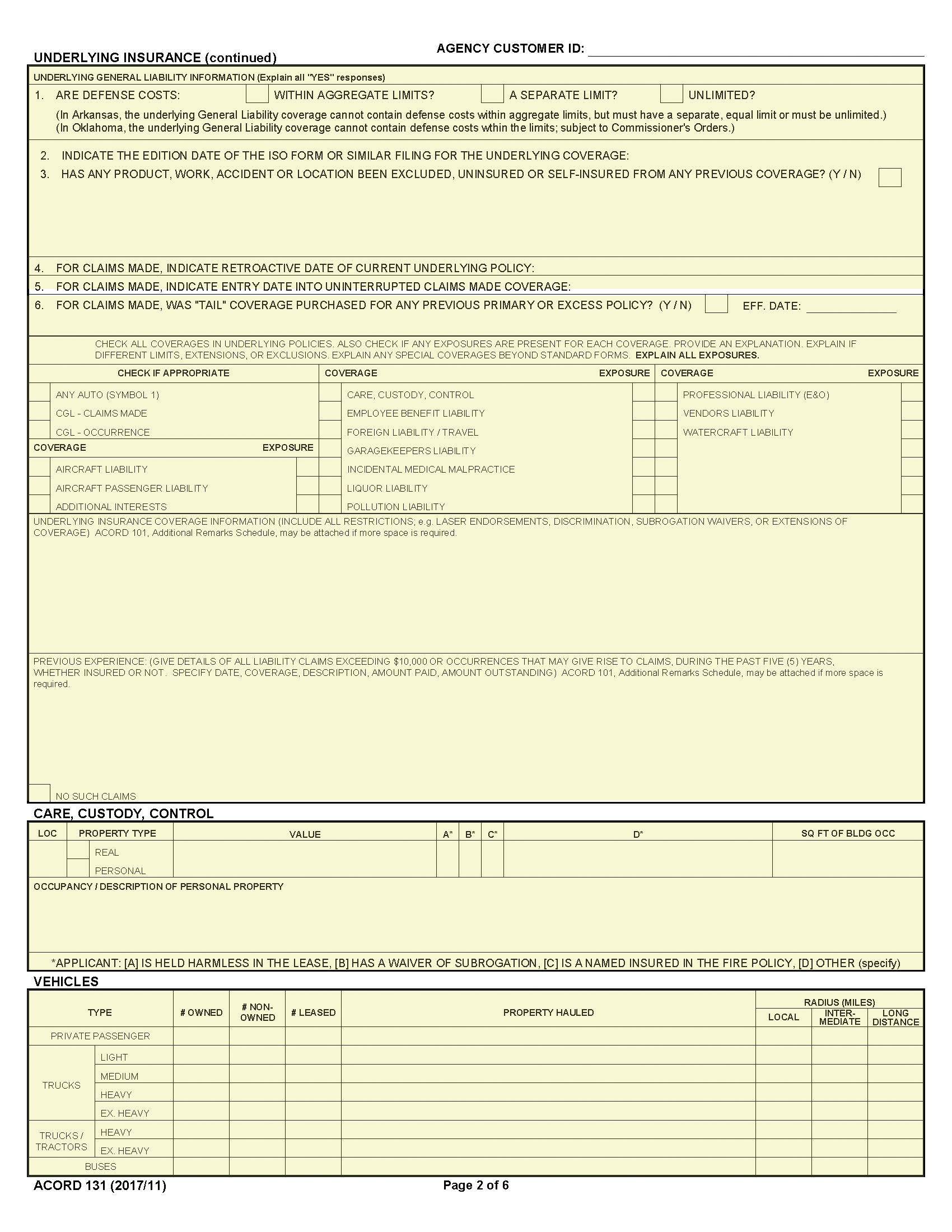
1. Underlying Insurance (continued)
Provide underlying General Liability Information requested. Explain all yes responses.
2. Coverage and Exposure Information
Check all coverages in underlying policies. Also check if any exposures are present for each coverage. Provide an explanation. Explain if different limits, extensions, or exclusions apply. Explain any special coverages beyond standard forms. Explain all exposures.
3. Care, Custody, Control
For property in the applicant’s care, custody or control provide the following information: Location number, property type (real or personal), value of that property, indicate whether applicant A. is held harmless in the lease; B. has a waiver of subrogation; C. is a named insured in the fire policy; D. Other (specify), square footage of the building occupied and describe the occupancy or the personal property.
4. Vehicles
Provide the type and number of vehicles owned, non-owned or leased. For each vehicle type, provide a description of the property hauled and radius of operation.
PAGE 3
Form Key
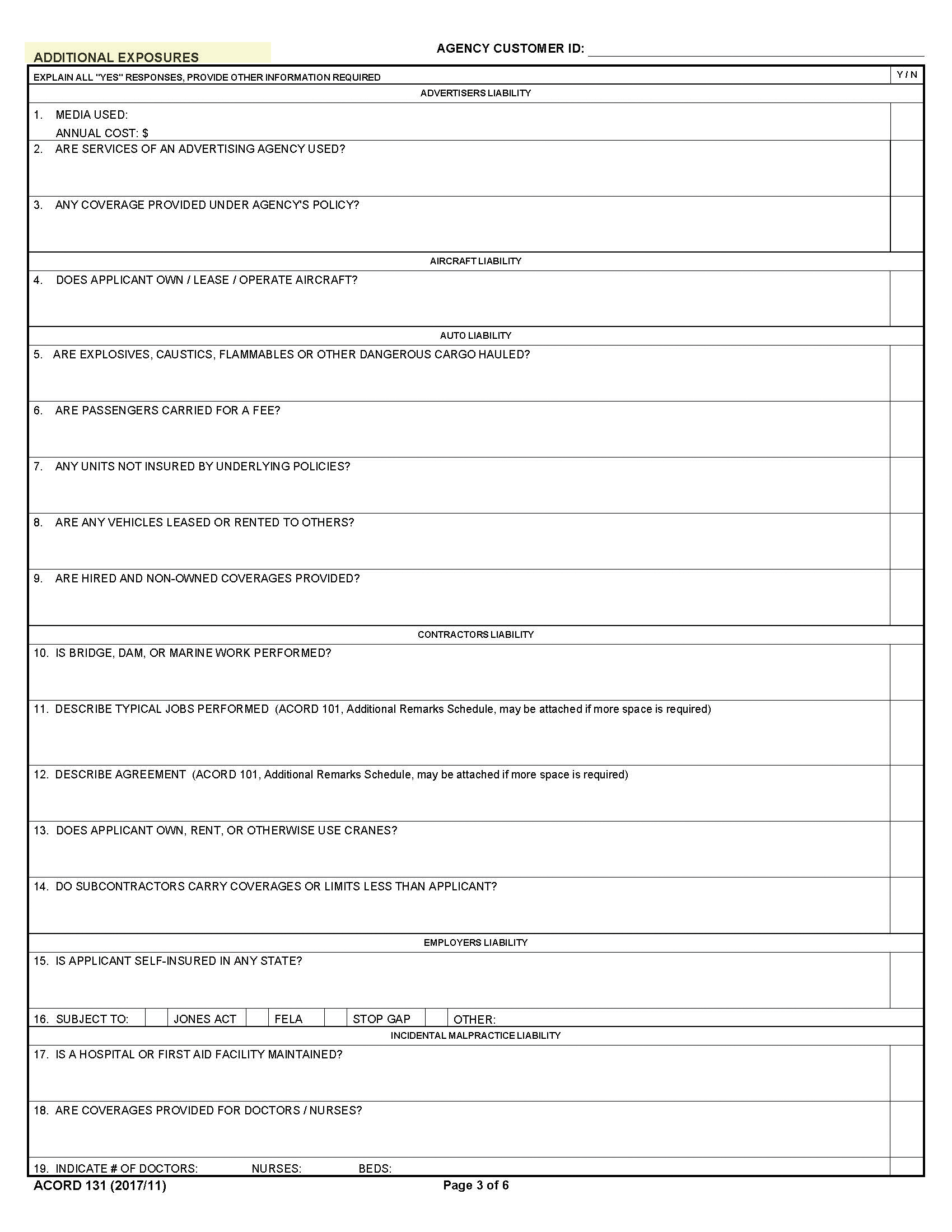
1. Additional Exposures
For each exposure provide the information requested. Explain all yes responses. Use the Remarks section on page 4 or use ACORD 101 if additional space is required.
PAGE 4
Form Key
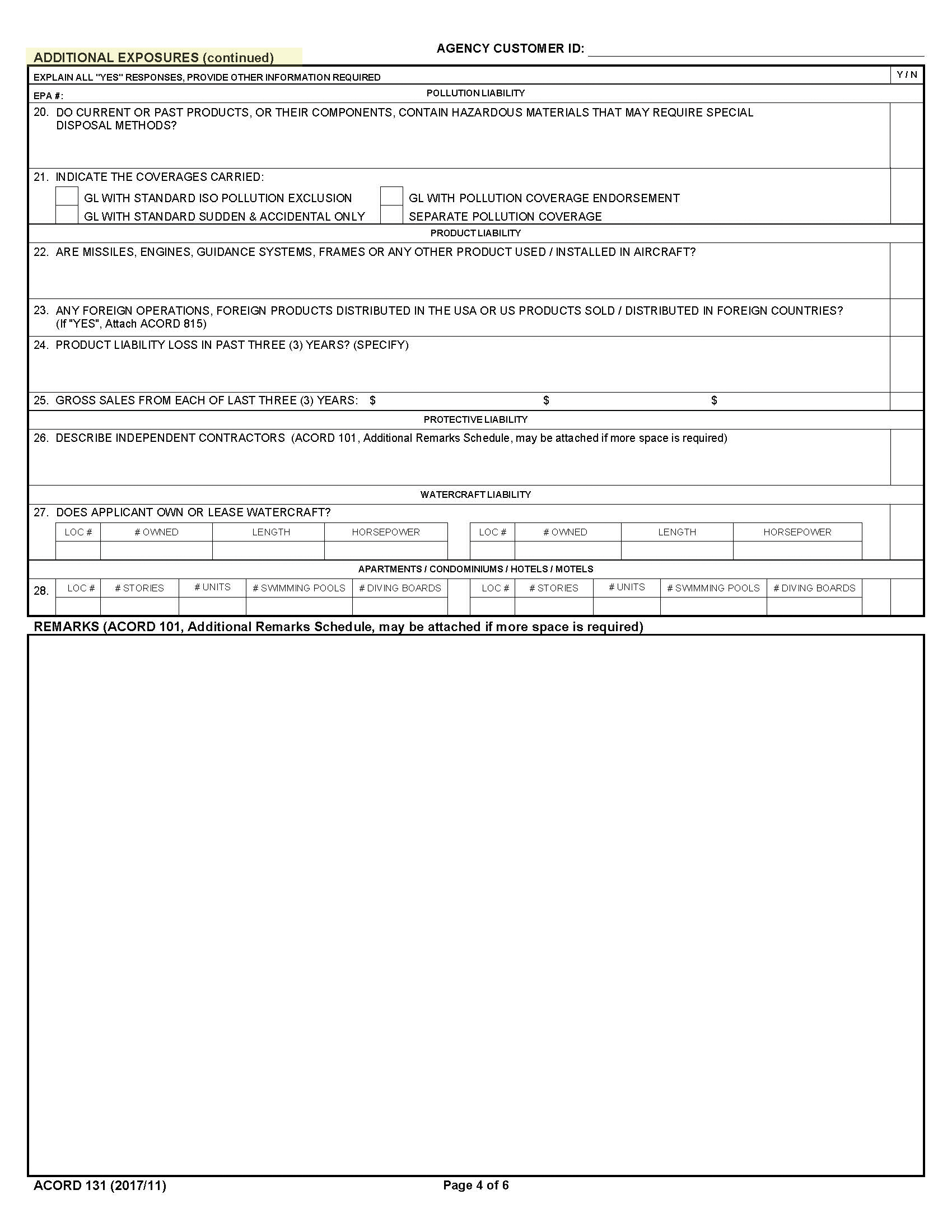
1. Additional Exposures (continued)
For each exposure provide the information requested. Explain all yes responses. Use the Remarks section below or use ACORD 101 if additional space is required.
PAGE 5

Form Key
1. Fraud Statements
This page displays the state specific Fraud Statements that apply to all applications for coverage.
PAGE 6
Form Key
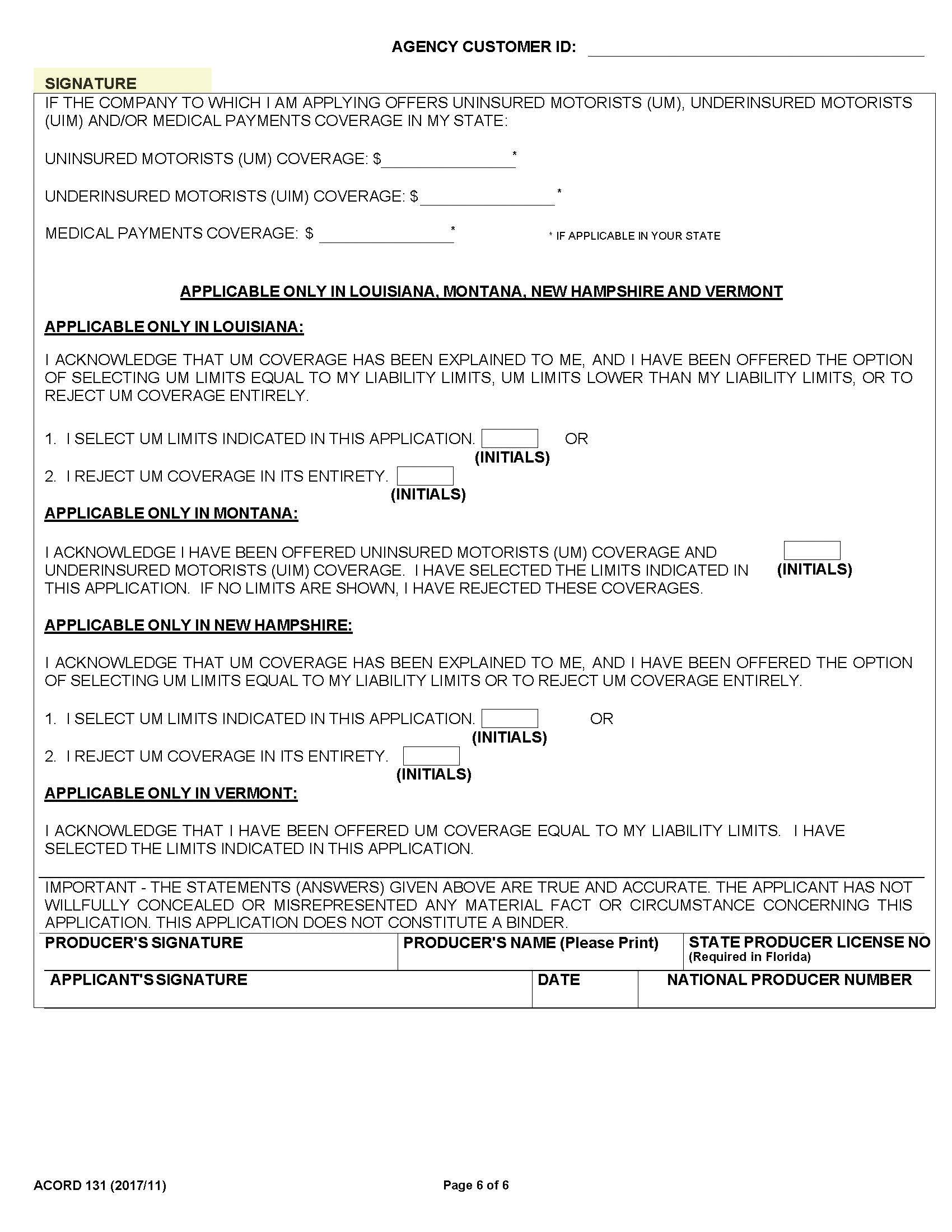
1. Signatures, date and Uninsured Motorist (UM), Underinsured Motorists (UIM) coverage and/or medical payments coverage selection.
Complete the applicable coverage selections for the applicant’s state. The producer and applicant must sign and date the application.
